
Scientific study on Chronic LBP

The effect of the Mastercare® Back-A-Traction® in combination with exercise therapy on chronic low back pain.
Study made from January to March 2003.
By physiotherapist: Karin Timmermans
© Mastercare AB
© Mastercare AB Only to be used for Mastercare products.
Please note: Studies not valid for "similar" products due to the big difference in function and usage.
Practical part
1. Introduction
In a Backcenter in Kalmthout near Antwerp (Belgium), the Mastercare – Back-A-Traction is being used for more then two years now (since 2001). One of the big advantages of this device is the possibility to work, under traction, in prone position, and perform some exercises to improve mobilization as well as stabilization of the lower lumbar segments. As up till now the results are very spectacular, it would be interesting to have a closer look at this treatment method.
The purpose of this study is to find out if these results can be confirmed scientifically. As subject of this study, the effect on pain and functional status in cases of chronic LBP was chosen. The participants underwent 10 treatments on the
Mastercare – Back-A-Traction. The effect was determined on the basis of VAS-scale and Oswestry LBP Disability Questionnaire.
This study was done from January till March 2003 at the Backcenter in Kalmthout (Antwerp-Belgium).
Research methodology
2.1 Patient selection
The inclusion criterion was chronic LBP. Patients were recruited sequentially as they presented at the centre.
Exclusion criteria:
– spinal disorder demonstrable on
plain radiograph (spondylolysis, listesis)
– cardiac insufficiency
– abdominal surgery
– glaucoma
– surgical intervention less then 6 months ago
– discodural & discoradicular interactions
with a high degree of inflammation
– presence of a tumour
– osteoporosis
– pregnancy
– high respiratory diseases
Important note: It has to be pointed out that these were exclusion criteria for this study (not to be confused with contra-indications for traction).
After receiving information about the goal of the study and their right to redraw at any time, patients gave their written consent to participate. None of the patients left the study.
Patients were allowed to keep on using their medication during the study but no changes were allowed.
Other co-interventions (as infiltrations, massage, electrotherapy, osteopathy, …) were not allowed.
2.2 Measuring-instruments
Before and after treatment, pain was measured using a 100 mm Visual Analogue Scale (VAS-scale) with a score of 0 (= no pain) to 100 (= unbearable pain), and the functional status of the patient was measured using the Oswestry LBP Disability Index.
These are standardized and validated measuring-instruments (11).
The correlation between these two instruments is moderate (r = 0.47 – 0.62). This is because pain and functional status are two different domains, which can not only be explained by a pathologic-anatomical or pathological-physiological point of view (29).
The measuring-instruments were taken by the physio- therapist before the first and after the tenth treatment.
Exactly six weeks after the last treatment, an Oswestry LBP Disability Questionnaire and a VAS-scale were sent towards the patients at home with the request to fill them in and to send them back
2.2.1 VAS-scale (appendix 1)
The VAS-scale is an instrument to measure the intensity of the pain (29). There is used a 100 millimetre visual analogue scale. The patient should mark on a line of 100 mm how he or she experiences her or his pain.
Left side of the line is no pain, right side is unbearable pain. The score lies between 0 and 100. The lower the score, the less pain our patient experiences
2.2.2 The Oswestry Low Back Pain Disability Questionnaire (appendix 2)
The Oswestry Low Back Pain Disability Questionnaire is an illness-specific questionnaire and gives us an image of the functional status of our patient (17,29).
The functional status gives us the restrictions the patient experiences in performing his daily activities (29).
The Oswestry Questionnaire encloses ten questions about subjects people with LBP can experience difficulties.
On every question the patient can choose out of 6 possible answers, but only one can be marked. When the patient doubt of several possibilities, he should mark what fits best.
For every part, score is minimal 0 and maximal 5. Score on the test varies from 0 to 50. This score will be multiplied by 2 and is expressed as a percentage of functional restriction (29).
The lower this percentage, the less restrictions our patient experiences during his daily activities.
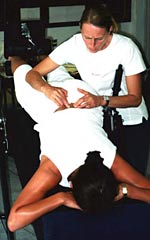
2.3 The Mastercare Back-A-Traction
The Mastercare – Back-A-Traction is a gravitational traction device with a unique moving backrest. It automatically stops at 0°, -15° and -30° inclination. This device makes it possible to exercise under traction and in prone position.
When we take a look at the essential points of therapeutically effective lumbar traction on this device, we find that, due to the moving backrest, with an inclination of 15°, the traction force is big enough to effect a structural change at the spinal segments, because the moving backrest eliminates friction. When we compare it to other inversion systems a much bigger inclination would be necessary to effect the same traction force.
This 15° we work in, is a very comfortable position and can be safely used for nearly all patients.
Principle of working
Before the patient steps into the Mastercare – Back-A-Traction, the right body-height has to be adjusted in order to have the right balance. Therefore the height and balance-adjustment knob has to be pulled out and the bar must be slided according to the guideline-markings provided. Unlocking one safety catch gives the therapist the possibility to make all adjustments from one side and to assist while inverting the table.
The table suits for people from 1.35 m till 2.15 m.

The patient will be secured by locking the foot restraint. Four pads around the ankles will fix the patient in a comfortable way during traction.

During the first treatment, the patient should get used to the device and to traction. We bring the table (and the patient) gently to the horizontal position and start with some breathing and relaxation exercises for optimal relaxation. As our organ of equilibrium is not used to this movement, the horizontal position won’t be registered correctly and the patient feels like inverted yet.

The support leg allows us to increase the inclination angle (and thus the traction) very slowly (from 0° to 15°). This is necessary in case of severe muscle spasm. On the other hand the support leg is used to stabilize the table when using mobilizations and or manipulations or other soft tissue techniques.


As to have the right inclination angle of 5° and 10°, before the start of the study, the table was gauged using a goniometre. Some markings were put on the support leg to point out how far exactly the support leg should be drawn out.

As to have the right inclination angle of 5° and+0 10°, before the start of the study, the table was gauged using a goniometre. Some markings were put on the support leg to point out how far exactly the support leg should be drawn out.
As for patient positioning, prone or supine, as both positions are possible on the table, it was the experience of the backcenter that prone position is a more comfortable position for most patients. So in the study all patients were treated in prone position


Prone position on the Mastercare – Back-A-Traction is not comparable with prone position on a common massage table or bed; the construction of the table allows knees and hips to stay in a light flexion during traction. The use of support pillows allows us to flex the hips even more to facilitate lumbar traction by flattening the lumbar spine. Also when stepping into and out of the Mastercare – Back-A-Traction, especially when there are disc problems involved, prone position shows to be a better position because we keep the neutral pelvic position, avoiding flexion of the lumbar spine when stepping out. If for one or another reason it is impossible to put the patient on the stomach and thus supine position is imposed, then a knee-support, individually adjustable, is available, which has to be used during the initial treatments.
The traction force is measured with the following formula:
Ftraction = W x sin a
In this formula W stands for the weight of the patient and astands for the angle of the table with the horizontal plane.
As the table is during the study maximum 15° inverted, we can easily determine the maximal traction force :
Ftraction = W x sin 15°
Ftraction = W x 0,26
Thus, using a 15° inclination:
Maximal traction force = 26 % of the bodyweight
2.4 The Treatment
The patients were treated daily on the Mastercare –
Back-A-Traction during 2 weeks; one treatment took approximately 45 minutes. If traction increased pain in the back or in the leg (which could signify that pain does not occur from a mechanical origin or that the degree of inflammation may be too big), the treatment should be stopped. All patients were treated with the same traction device.
During the treatment a protocol was followed. This study protocol was approved by the Medical Ethics committee of the University department of Physiotherapy in Antwerp (Belgium). In this protocol treatment from day 1 till day 10 was written out completely.
Protocol
Day 1:
– The patient comes in after making an appointment;
– The patient receives information about the device
and the study;
– The written consent to participate is asked;
– The VAS-scale and Oswestry questionnaire are taken;
– Anamneses and functional examination are taken;
– Initial treatment : getting the patient familiar with the device and traction;
– The patient is positioned depending his or her status.
We keep the patient for at least 5 minutes in the samenposition, except when the patient feels uncomfortable or is in pain. First our patient lies in the horizontal position, positioned pain free if possible, and breathing is checked. Then we invert our patient in 5° inclination, using the support leg and our patient should be able to carry out an abdominal breathing without increasing the pain. This position is followed by 3 minutes in horizontal position, making walking movements with the legs.

Then we increase the inclination-angle progressively, 5 minutes traction in 10° (support leg), followed by 3 minutes horizontal, till we have our patient in 15° (automatic stop), using some times manual techniques if necessary to relieve pain and to take muscle spasm away
As for patient positioning, prone or supine, as both positions are possible on the table, it was the experience of the backcenter that prone position is a more comfortable position for most patients. So in the study all patients were treated in prone position


During traction, the patient should be able to carry out an abdominal breathing. Is this breathing still painful then we ask to breath within the pain limit. During all the following treatments the patient is asked to carry out an abdominal breathing. Initially this breathing might be difficult especially in prone position. Therefore you instruct this breathing before starting on the table. Breathing this way gives us a good idea of the status of the lumbar segments.
When we put the table back into the starting position, this should be carried out very slowly and we ask the patient to keep on making a walking movement by alternate bending the knees in a slow and easy walking motion. This way the pressure on the discs stays variable. After stepping out of the Mastercare – Back-A-Traction it’s very important to relax and to take it easy for a few minutes (walk around for 5 minutes). Lifting weights and strenuous movements must be avoided immediately after traction.
The average length of treatment, counting the non-continuous character of traction during the first sessions, is more or less 45 minutes.
Patients also receive a limited back schooling during first treatments.
Day 2:
– We built up traction progressively, same as Day 1, and start mobilization exercises on the table.
– Breathing out, pushing both heels backward (dorsiflex), at the same moment contracting M.Transversus Abd. and straightening legs as to contract Quadriceps and Tibalis Anterior. Repeat 7 times.
– Also alternating right, left heel depending on the condition treated, sometimes only right or left.



– Extension mobilizations : the patient lies for 3 X 1 minute in elbow-support with 20 seconds rest in between. Always pushing up symmetrically.


– Our patient lies down for 3 minutes and then he’s asked to push up 3 times for 1 minute on straight arms (hips should stay on the table). This should not be painful, otherwise the patient should stay lower.

– Put the patient back to the horizontal position where he stays a few minutes making walking movements. Then gently bring the patient back in the starting position.

Day 3:
– Same as Day 2, although we invert immediately to 15°, repeating the same exercises as Day 2. We add dynamic extension exercises : the patient should push up on straight arms and repeat 2 X 10 push ups.
– We start lumbar stabilization training (contraction of TA and lumbar multifidi). During breathing out (abdominal breathing) we ask to contract the TA and raise head and shoulders slightly during 3 seconds. Repeat 2 X 10.
Day 4:
– Same as Day 3, all exercises are repeated. We add :
– Consciously contracting the musculi multifidii. During breathing out we ask the patient to contract the TA and slightly hollow the lower back, without relaxing the abdominals. As feedback we control the musculi multifidii with the fingertips just besides the spine.
Day 5:
– All exercises of Day 4 are to be repeated.
– The stabilization-exercises are enlarged to 3 X 10.
Day 6 till Day 9:
– The treatment remains the same as on Day 5.
Day 10:
– The treatment remains the same.
– The VAS-scale and Oswestry Questionnaire are taken again.
The Research- and measuring results + statistical processing
3.1. The Research- and measuring results
For this study 15 patients gave their written consent to participate. The subjoined schedule gives us the characteristics of the study population.
The average age was 45,5 years. The youngest person was 36 years old and the oldest person was 60 years old.
There were 9 women and 6 men who participated the study.
Three persons are to be considered as completely disabled (unfit for work) and lived from disability benefit.
Eight patients had radiation pain towards 1 leg, 2 patients towards both legs. Five patients had no radiation pain.
Only 1 patient had less then 1 year complaints. Four patients had less then 5 years complaints and 5 less then 10 years. Five people suffered longer then 10 years from LBP. The average duration of the LBP was 9,96 years.
12 out of the 15 patients had a disturbed night’s rest.
9 patients had complaints due to a pathology of the intervertebral disc. In one case this was due to a spinal disorder (n=1), fibromyalgia (n=1) or narrowed neuroforamina (n=1). 3 patients suffered from aspecific LBP.
All patients had tried out one or more different treatments. Physiotherapy and infiltration (n=10) were the most popular, followed by osteopathy (n=7).
3.2. The statistical processing
All patients completed the study. In all cases measuring instruments were taken before the first and after the tenth treatment by the physiotherapist.
Six weeks after the end of the treatment there were some drop-outs. Four people did not send back the Oswestry Questionnaire and the VAS-scale and in one case results were not completed.
The subjoined table shows us the results.
The results were partly processed by Sigmastat and partly by Microsoft Excel. For all specific operations by Sigmastat and the graphic processing is referred to appendix 3, 4 and 5.
3.2.1. The VAS-scores
First the results of the VAS-scale were compared. Subjoined table shows us the VAS-score before, after and 6 weeks after treatment :

Only 1 patient had a higher VAS-score after treatment then before. His score on the Oswestry Questionnaire remained the same.
The average score decreased from 68,267 before the treatment to 32,867 after treatment. The highest and lowest scores also decreased. The maximum score fell from 99,000 to 89,000 and the minimum score from 27,000 to 0,000. The VAS-score after treatment decreased with an average of 35,400.
If we look at the results 6 weeks after the study, we see that the average score decreased even more till 26,600. The maximum score decreased till 70,000.
From the 10 people who responded by sending back the Questionnaire and the VAS-scale, 5 continued to follow the treatment after the study was finished. Three of these patients had a lower VAS-score right after the end of the treatment (one followed the treatment daily, the two others 2 and 3 times a week). In two other cases VAS-score was slightly increased (they proceeded treatment but only once a week).
Among the 5 patients who did not proceed the treatment, we saw in one case a lower VAS-score after 6 weeks in comparison with right after treatment. For 3 people the score was higher and for 1 person the score remained 0.
To know the effect on pain of this treatment, VAS-score before and after treatment were compared. Therefore the softwareprogramm Sigmastat was used.
The results were first compared by means of a Paired t-test. This proved that there is a statistical significant difference (p<0,01).
Due to the low number of results (n<30) it was advised to use an Unpaired t-test.
Therefore, with the help of Sigmastat, the Wilcoxon Signed Rank test was used. This test also proved that there is a statistical significant difference (p<0,01).
If we compare the starting results with the results of 6 weeks after treatment we get with the Paired t-test a p<0,01. When we use the Wilcoxon Signed Rank test, we can see that Sigmastat automatically runs a Paired t-test. This happens because Sigmastat finds the data much better ordered for the Paired t-test then for the Wilcoxon Signed Rank test. There is a statistical significant difference between both data with a p<0,01.
As conclusion we can point out that the positive effect of the treatment on pain is bigger then by chance alone. This is the case right after treatment as after 6 weeks after the end of treatment.
3.2.2. The Oswestry Low Back Pain Disability Index
Here the results of the Oswestry LBP Disability Questionnaire are discussed.
Subjoined table shows us the results of the Oswestry Questionnaire :

In one case the Oswestry score was higher after the study then by the start (fibromyalgia patient), althought the VAS-scale pointed out a lower score. In another case the Oswestry score remained exactly the same before and after treatment.
Six weeks after the end of the study 4 of the 10 patients had a lower Oswestry LBP Disability Index then right after the study. In case of 5 patients it was higher and in 1 case it remained the same.
The average decreased from 44,400 before treatment to 23,800 right after and to 20,700 six weeks after treatment.
To trace the effect of this particular treatment on the functional status of the patient, we compared again the results of the Oswestry LBP Disability Index before and after treatment.
Also here we used Sigmastat. As well the Paired t-test as the Wilcoxon Signed Rank test showed a statistical significant difference with a p<0,01.
If we compare the startingresults with the data from 6 weeks after treatment, we see a p>0,01, but it’s still smaller then 0,05. There’s still a statistical significant difference. Also here Sigmastat automatically ran the Paired t-test when asked to execute the Wilcoxon Signed Rank test.
The effect of the treatment on the functional status of the patient is bigger then by chance alone. The influence of the treatment on the functional status is therefore positive and this as well right after as six weeks after the treatment.
3.2.3. The relation between the results of VAS-scale and the Oswestry LBP Disability Index.
To know the relation between the two used measuringinstruments, we must calculate the correlation between both. Therefore we used the Spearman Rank Order Correlation via Sigmastat.
The correlationcoefficient before the study is 0,735, after the study 0,507 and six weeks after the study 0,979.
The correlation between the two measuringinstruments before and after the study is moderate.
Six weeks after the end of the treatment there’s a high correlation.
Discussion
This research gives us positive results. The suggested treatment has a positive effect on the pain and the functional status of chronic LB patients.
The results of this study are in contradiction with some authors’ views. As to these authors lumbar traction has only a positive effect in the acute stage of LB problems and in the chronic stage best results are achieved by active treatmentformula (30, 46).
We might ask ourselves whether the effect of this treatment is due to the traction, to the exercise therapy or is it the combination of both? Therefore it would be interesting to execute this study again but with 2 control groups where we divide the patients at random. One group with only traction and a second with only the exercises as treatment. A third group with the treatment as it was executed in this study.
To compare the results of this study with other data out of literature is not possible because of the following reasons :
– There are no studies where traction has been performed in prone position;
– There are no studies where exercises are given under traction;
Another limitation is the rather small, not homogeneous study population. The results of this study should have a bigger reliability if we would have tested a bigger and more homogeneous population.
Six weeks after the end of the treatment there were only results of 10 patients. These results can be compared but don’t give us a complete and correct image because :
– Not everybody continued to follow the treatment;
– If the treatment was continued, there was a difference in frequency.
When we look at the correlation between both measuring instruments we see that only after the treatment our value (r=0,507) lies in between the supposed 0,470 and 0,620 (29). Before the treatment (r=0,735) and six weeks after the end of the treatment (r=0,979) this value lies above the 0,620. A possible cause is the small heterogeneous study population.
Not only about the results of the study but also about the Mastercare – Back-A-Traction and the use of it we can make some remarks :
– The device was gauged in a rather rudimentary way.
There’s a possibility that during the gauging some measuring mistakes were made, although this has no influence on the results as all the patients have been treated on the same device.
– It’s important to inverse the table gently. When we don’t do this it’s possible that muscles contract by reflex against the abrupt stretching.
– During traction the patient is fixated by the ankles. Therefore we also find a traction in ankle-, knee- and hip joints. A few patients (n=5) found the traction in the ankle joints in the beginning of the treatment rather uncomfortable, but after a few sessions there were no complaints no more.
– When stepping out of the Mastercare – Back-A-Traction some patients (n=4) experienced disequilibrium. We just have to see that the patient is put back step by step giving the organ of equilibrium time to registrate this movement correctly.
– Theoretically the maximal tractionforce on the lower lumbar spine is 26% of the bodyweight. Practically this is not the case as we might have a very slightly loss due to friction, but most of all as a part of the tractionforce is executed on other joints (ankle, knee, hip).
– In literature no one agrees about the optimal tractionforce. Pellechia describes the necessity of tractionforces between 10 % and 300 % of the bodyweight (40). According to Heijden et al a tractionforce of at least 20 % of the bodyweight should be necessary to result in a positive and clinical effect on the lumbar spine (49).
– Comparing duration and frequency of the treatment with existing data in literature is also impossible because there are no studies evaluating these parameters (30, 40, 49).
General conclusion
Out of the study of literature it seemed that almost all randomized clinical trials about lumbar traction showed methodical shortcomings. The methodical strong studies showed however no positive effect.
Until now conclusions can not be drawn if lumbar traction would be more effective than other treating methods. Although there is no evidence that traction would be ineffective for the treatment of low back pain. Further research is necessary.
If the supposed effects of lumbar traction were critically looked at, we saw that a lot of these so called effects based on ill-founded hypotheses.
The scientifical study proved that the proposed treatment resulted in a positive effect on pain and functional status of chronic low back patients, but further research is also necessary.
It is recommended to repeat this study but with a larger population divided into 3 groups : one group only using traction, a second group only executing the exercises and a third group, as presented in this study, executing the exercises under traction.
It could be considered to repeat this research to know the effect on a certain, homogenous population. For example only patients with a specific low back complaints can be admitted to the study.
The subject of this study was the effect on pain and the functional status of the patient, but it would also be interesting to know the effect on mobility. This could also be investigated in future.
Abstract
The effect of gravity muscle traction combined with an exercise therapy on chronic low backpain
Introduction:
The Backcenter in Kalmthout (Antwerp-Belgium) uses since 2001 an interesting traction-device. They’ve obtained spectacular results with it. The Mastercare – Back-A-Traction makes it possible to give exercise therapy in traction and in prone position.
Goal:
To trace the effect of this combination therapy on pain and the functional status of chronic low back patients.
Method:
Only patients with backpain for more then 12 weeks were admitted to the study. The test persons underwent 10 treatments with a frequency of 5 times a week on the Mastercare – Back-A-Traction. The evaluation was done with the VAS-scale and the Oswestry Low Back Pain Disability Questionnaire, which were taken by the physiotherapist before the first and after the last treatment. Six weeks after the end of the treatments, the patients received the same papers by post with the question to fill them in and to sent them back.
Results:
15 persons enrolled for the study. Right after the treatment as after 6 weeks we can see a positive effect on pain (p<0,01). After 10 treatments we see that there was also a positive effect on the functional status (p<0,01). Six weeks after the last treatment the p-value was increased but still under 0,05. So we can state that this treatment method has a positive effect on pain and functional status on chronic low back patients.
Discussion:
The results of this study are in contradiction with the opinion that traction has only a positive effect in the acute stage. The question arises whether these positive effects were caused by the traction, by the exercise therapy or by the combination of both. Because of the absence of control groups, an answer cannot be given. Another limitation of this research is the small, not homogenous study population.
Conclusion:
Although the results of this study are positive, they should be considered with some reserve. Because of the limited methodology, this way of treatment may not be seen as a new wonder technique. It is recommended to repeat this study with a larger study population and the presence of control groups.
Appendix
APPENDIX 1
THE VISUAL ANALOGUE SCALE
The patient makes a mark across the line below to indicate the pain he or she’s experiencing at the moment. On the left side of the line the patient experiences no pain at all, on the right side the pain is unbearable.
APPENDIX 2
THE OSWESTRY LOW BACK PAIN DISABILITY QUESTIONNAIRE.
Part 1 : Pain Intensity
I can tolerate the pain I have without having to use pain killers.
The pain is bad but I can manage without pain killers.
Pain killers give complete relief of pain.
Pain killers give moderate relief of pain.
Pain killers give very little relief of pain.
Pain killers have no effect on the pain, so I’m not using them.
Part 2 : Personal Care (washing, dressing)
I can look after myself normally without causing extra pain.
I can look after myself normally but it causes extra pain.
It is painful to look after myself and I am slow and careful.
I need some help but manage most of my personal care.
I need help every day in most aspects of self-care.
I do not get dressed, wash with difficulty and stay in bed.
Part 3 : Lifting
I can lift heavy weights without extra pain.
I can lift heavy weights but it gives extra pain.
Pain prevents me from lifting heavy objects off the floor,
but I manage if they are conveniently positioned e.g. on a table.
I can only lift very light weights.
I cannot lift or carry anything at all.
Part 4 : Walking
Pain does not prevent me from walking any distance.
Pain prevents me from walking more than 2 kilometer.
Pain prevents me from walking more than 1 kilometer.
Pain prevents me from walking more than 500 meter.
I can only walk using a stick or crutches.
I am in bed most of the time and have to crawl to the toilet.
Part 5 : Sitting
I can sit in any chair as long as I like.
I can only sit in my favorite chair as long as I like.
Pain prevents me from sitting more than an hour.
Pain prevents me from sitting more than 30 minutes.
Pain prevents me from sitting more than 10 minutes.
Pain prevents me from sitting at all.
Part 6 : standing
I can stand as long as I want without extra pain.
I can stand as long as I want but it gives extra pain.
Pain prevents me from standing more than an hour.
Pain prevents me from standing more than 30 minutes.
Pain prevents me from standing more than 10 minutes.
Pain prevents me from standing at all.
Part 7 : Sleeping
Pain does not prevent me from sleeping well.
I can sleep well only by using tablets.
Even when I take tablets I have less than 6 hours sleep.
Even when I take tablets I have less than 4 hours sleep.
Even when I take tablets I have less than 2 hours sleep.
Pain prevents me from sleeping at all.
Part 8 : Sex Life
My sex life is normal and causes no extra pain.
My sex life is normal but causes some extra pain.
My sex life is normal but is very painful.
My sex life is very restricted because of pain.
My sex life is nearly absent because of pain.
Pain prevents any sex life at all.
Part 9 : Social Life
My social life is normal and gives me no extra pain.
My social life is normal but increases the degree of pain.
Pain has no significant effect on my social life,
apart from limiting my more energetic interests, e.g. dancing.
Pain has restricted my social life and I do not go out as often.
Pain has restricted my social life to my home.
I have no social life because of pain.
Part 10 : Traveling
I can travel anywhere without pain.
I can travel anywhere but it gives me extra pain.
Pain is bad but I manage journeys over 2 hours.
Pain restricts me to journeys of less than 1 hour.
Pain restricts me to short, necessary journeys of under 30 minutes.
Pain prevents me from traveling except to the doctor or the hospital.
APPENDIX 3
GRAPHICAL PROCESSING OF THE RESULTS
Appendix 4
STATISTICAL PROCESSING OF VAS-SCALE
A) Before and right after treatment
PAIRED T-TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P > 0.200).
t = 6.000 with 14 degrees of freedom. (P = < 0.001).
95 percent confidence interval for difference of means : 22.746 to 48.054.
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant change (P = < 0.001).
Power of performed test with alpha = 0.050 : 1.000.
WILCOXON SIGNED RANK TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P > 0.200).

W = -116.000 T+ = 2.000 T- = -118.000 P(est.) = 0.001 P(exact) = <0.001 .
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant difference (P = < 0.001).
B) Before and 6 weeks after treatment
PAIRED T-TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P = 0.150).

t = 3.944 with 9 degrees of freedom. (P = 0.003).
95 percent confidence interval for difference of means : 15.567 to 57.433 .
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant change (P = 0.003).
Power of performed test with alpha = 0.050 : 0.934 .
WILCOXON SIGNED RANK TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P = 0.150).
Test execution ended by user request, Paired t-test begun
Paired t-test : Wednesday, May 07, 2003, 14:08:10 .
Data source : data 1 in Notebook.

t = 3.944 with 9 degrees of freedom. (P = 0.003).
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant change (P = 0.003).
APPENDIX 5
STATISTICAL PROCESSING OSWESTRY LOW BACK PAIN DISABILITY QUESTIONNAIRE
A) Before and right after treatment
PAIRED T-TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P > 0.200).
t = 6.000 with 14 degrees of freedom. (P = < 0.001).
95 percent confidence interval for difference of means : 22.746 to 48.054 .
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant change (P = < 0.001).
Power of performed test with alpha = 0.050 : 1.000 .
WILCOXON SIGNED RANK TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P > 0.200).
Test execution ended by user request, Paired t-test begun
Data source : Data 1 in Notebook

t = 4.697 with 14 degrees of freedom. (P = <0.001)
95 percent confidence interval for difference of means : 11.193 to 30.007
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant change (P = <0.001).
B) Before and 6 weeks after treatment
PAIRED T-TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P = 0.143).
t= 2.914 with 9 degrees of freedom. (P = 0.017).
95 percent confidence interval for difference of means : 4.633 to 36.767 .
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant change (P = 0.017).
Power of performed test with alpha = 0.050 : 0.688 .
The power of the performed test (0.688) is below the desired power of 0.800 .
You should interpret the negative findings cautiously.
WILCOXON SIGNED RANK TEST
Data source : Data 1 in Notebook.
Normality Test : Passed (P = 0.143).
Test execution ended by user request, Paired t-test begun.
Paired t-test : Wednesday, May 07, 2003, 14:27:12 .
Data source : Data 1 in Notebook.
t= 2.914 with 9 degrees of freedom. (P = 0.017).
95 percent confidence interval for difference of means : 4.633 to 36.767 .
The change that occurred with the treatment is greater than would be expected by chance; there is a statistically significant change (P = 0.017).
References
BOOKS
(1) BENNO, M.N. and HERZOG, W., Biomechanics of the Musculo-skeletal System, Wiley, Chichester, 1994, p. 47-198.
(2) BOGDUK, N., Clinical Anatomy of the Lumbar Spine and Sacrum, 3de druk, Churchill Livingstone, Edinburgh, 1997, p. 67-101.
(3) CAILLIET, R., Low Back Pain Syndrome, F.A. Davis Company, Philadelphia, 1988.
(4) CYRIAX, J., Textbook of Orthopaedic Medicine Vol.1, 7de druk, Bailliere Tindall, London, 1980.
(5) FORDYCE, W.E., Back pain in the work place, IASP Press, Seattle, 1995.
(6) GRIEVE, G., Common vertebral joint problems, Churchill Livingstone, Edinburgh, 1981.
(7) KAPANDJI, I.A., Bewegingsleer deel 3 : de romp, 1e druk, Bohn Stafleu van Loghum, Houten, 1997, p. 20-23.
(8) Mc KENZIE, R., The lumbar spine, Spinal Publications, Waikanae, 1981.
ARTICLES FROM MAGAZINES
(9) ANDERSSON, G.B.J., SCHULTZ, A.B. and NACHEMSON, A.L., Intervertebral disc pressures during traction, Scandinavian Journal of Rehabilitation Medicine, 1983, p. 88-91.
(10) BEURSKENS, A.J.H.M., e.a., Efficacy of traction for non-specific low back pain. 12-week and 60 month results of a randomised clinical trial, Spine, 1997, 22, p. 2756-2762.
(11) BEURSKENS, A.J.H.M., DE VET, H.C.W., KÖKE, A.J.A., and VAN DER HEIJDEN, G.J.M.G., Measuring the functional status of patients with low back pain. Assessment of the quality of four disease-specific questionnaires, Spine, 1995, 20, p. 1017-1028.
(12) BIHAUG, O., Autotraksjon for ischialgpasienter : en kontrollert sammenlikning mellom effekten av auto-traksjon og isometriske ovelser ad modum hume endall og enkins, Fysioterapeuten, 1978, 45, p. 377-379.
(13) BLIX, M., Die Laenge und die Spannung des Muskels, Skand. Arch. Physiol., 1894, 5, p. 149-206.
(14) BRIDGER, R.S., OSSEY, S. and FOURIE, G., Effect of lumbar traction on stature, Spine, 1990, 156, p. 522-524.
(15) COLACHIS, S.C., and STROHM, B.R., Effects of intermittent traction on separation of lumbar vertebrae, Archives of Physical Medicine and Rehabilitation, 1969, 44, p. 251-25/.
(16) COXHEAD, C.E., INSKIP, H. and MEADE, T.W., Multicentre trial of physiotherapy in the management of sciatic symptoms, Lancet, 1981, p. 1085-1088.
(17) FAIRBANK, J.C.T., COOPER, J. DAVIES, J.B. and O’BRIEN, J.P., The Oswestry low back pain disability questionnaire, Physiotherapy, 1980, 66, p. 271-273.
(18) GORDON, A.M., HUXLEY, A.F. and JULIAN, F.J., The variation in isometric tension with sarcomeren length in vertebrate muscle fibres, Journal of Physiology, 1966, 184, p. 170-192.
(19) GREEN, T.P., ADAMS, M.A., and DOLAN, P., Tensile properties of the anulus fibrosus II, European Spine Journal, 1993, 2, p. 209-214.
(20) GRÖNBLAD, M., e.a. Straight leg raising test and lumbar cerebrosipinal fluid levels of vasoactive intestinal peptide and somatostatin in patients with low back pain, Spine, 1994, 19, p. 1462-1466.
(21) GUPTA, R. and RAMARAO, S., Epidurography in reduction of lumbar disc prolapse by traction, Archives of Physical Medicine and Rehabilitation, 1978, 59, p. 322-327.
(22) HALL, T., ZUSMAN, M., and ELVEY, R., Adverse mechanical tension in the nervous system ? Analysis of the straight leg raise, Manual Therapy, 1998, 3, p. 140-146.
(23) HASKVITZ, E.M., and HANTEN, W.P., Blood pressure response to inversion traction, Physical Therapy, 1986, 66, p. 1361-1364.
(24) HASUE, M., Pain in the nerve root : an interdisciplinary approach, Spine, 1993, 14, p. 2053-2058.
(25) HICKLING, J., Spinal traction technique, Physiotherapy, 1972, 58, p. 58-63.
(26) JAYSON, M.M., The role of vascular damage and fibrosis in the pathogenesis of nerve root damage, Clinical Orthopaedics and Related Research, 1992, 279, p. 40-48.
(27) JUDOVICH, B.D., Lumbar traction therapy – Elimination of physical factors that prevent lumbar stretch, Journal of the American Medical Association, 1955, 159, p. 549-550.
(28) KNUTTSON, E., SKOGLUND, C., and NATCHEV, E., Changes in voluntary muscle strength, somatosensory transmission and skin temperature concomitant with pain relief during autotraction in patients with lumbar and sacral root lesions, Pain, 1988, 33, p. 173-179.
(29) KÖKE, A.J.A., BEURKENS, A.J.H.M. and DE VET, H.C.W., Meten van activiteitsniveau bij patiënten met lage rugklachten. De functionele status., Ned. T. Fysiother., 2001, 111, p. 74-78.
(30) KRAUSE, M., REFSHAUGE, M. DESSEN, M. and BOLAND, R., Lumbar spine traction : evaluation of effects and recommended application for treatment, Manual Therapy, 2000, 5, p. 72-81.there is a statistically significant change (P = 0.017).
ARTICLES FROM MAGAZINES CONT.
(31) LARSSON, U., e.a., Auto-traction for treatment of lumbago sciatica, Acta Orthopaedica Scandinavica, 1980, 51, p. 72-81.
(32) LIDSTRÖM, A., and ZACHRISSON, M., Physical therapy on low back pain and sciatica, Scandinavian Journal of Rehabilitation Medicine, 1970, 2, p. 37-42.
(33) LJUNGRENN, E., WEBER, H., and LARSSEN, S., Autotraction versus manual traction in patients with prolapsed lumbar intervertebral discs, Scandinavian Journal of Rehabilitation Medicine, 1984, 16, p. 117-124.
(34) MATHEWS, J.A., Dynamic Discography : a study of lumbar traction, Annals of Physical Medicine, 1968, 9, p. 275-279.
(35) MATHEWS, J.A. and HICKLING, J., Lumbar traction : a double-blind controlled study for sciatica, Rheumatology Rehabilitation, 1975, 14, p. 222-225.
(36) MARKOLF, K.L., Deformation of the thoracolumbar intervertebral joints in response to external loads, J. Bone Joint Surgery, 1972, p. 511-533.
(37) NACHEMSON, A., Newest knowledge of low back pain : a critical look, Clinical Orthopaedics and Related Research, 1992, 279, p. 8-20.
(38) ONEL, D., TUZACI, M., SARI, H. and DEMIR, K., Anulus tears and intervertebral disc degeneration : an experimental study using an animal model, Spine, 1989, 15, p. 762-767.
(39) PAL, B., MANGION, P., HOSSAIN, M.A. and DIFFEY, B.L., A controlled trial of continuous lumbar traction in the treatment of back pain and sciatica, British Journal of Rheumatology, 1986, 25, p. 181-183.
(40) PELLECHIA, L.G., Lumbar Traction : A Review of the Literature, Journal of Sports and Physical Therapy, 1994, 20, p. 262-267.
(41) REUST, P., CHANTRAINE, A., and VISCHER, T.L., Traitement par tractions mecaniques des lombosciatalgies avec ou sans deficit neurologique, Schweiz Med Wochenschr., 1988, 118, p. 271-274.
(42) SAUNDERS, H.D., Use of spinal traction in the treatment of neck and back conditions, Clinical Orthopaedics, 1983, 179, p. 31-37.
(43) SKAGS, D.L., WEIDENBAUM, M., IATRIDIS, J.C. and RATCLIFFE, A., Regional variation in tensile properties and biomechanical composition of the human lumbar anulus fibrosus, Spine, 1994, 19, p. 1310-1319.
(44) SMITH, S.A., MASSIE, J.B., CHESTNUT, R. and GARVIN, S.R., Straight leg raising : anatomical effects on the spinal nerve root without and with fusion, Spine, 1993, 18, p. 992-999.
(45) TESIO, L., LUCCARELLI, G. and FORNARI, M., Natchev’s auto-traction for lumbago-sciatica : effectiveness in lumbar disc herniation, Archives of Physical Medicine and Rehabilitation, 1989, 70, p. 831-834.
(46) TULDER, M.W. VAN, KOES, B.W. and BOUTER, L.M., A cost-of-illness study of back pain in the Netherlands, Pain, 1995, 62, p. 232-240.
(47) TWOMEY, L.T., Sustained lumbar traction. An experimental study of long spine segments, Spine, 1985, 10, p. 146-149.
(48) VAN DER HEIJDEN, G.J.M.G., e.a., The efficacy of traction for back and neck pain : a systematic, blinded review of randomised clinical trial methods, Physical Therapy, 1995, 75, p. 93-104.
(49) VAN DER HEIJDEN, G.J.M.G., BOUTER, L.M., and TERPSTRA-LINDEMAN, E., De effectiviteit van tractie bij lage rugklachten : de resultaten van een pilotstudy, Ned. T. Fysiotherapie, 1991, 101, p. 37-43.
(50) WALKER, L., SVENKERUD, T. and WEBER, H., Traksjonsbehandling ved lumbago-ischias, Fysioterapeuten, 1982, 49, p. 271-274.
(51) WATKINS, L.R. and MAYER, D.J., Organization of endogenous opiate and nonopiate pain control systems, Science, 1982, 216, p. 1185-1192.
(52) WEBER, H., Traction therapy in sciatica due to disc prolapse, Journal of the Oslo City Hospital, 1973, 23, p. 167-176.
(53) WEBER, H., LJUNGREN, E. and WALKER, L., Traction therapy in patients with herniated lumbar intervertebral discs, Journal of the Oslo City Hospital, 1984, 34, p. 61-70.
(54) YATES, D., Indications and contraindications for spinal traction, Physiotherapy, 1972, 58, p. 55-57.
(55) ZITO, M., Effect of two gravity inversion methods on heart rate, systolic brachial pressure, and ophthalmic artery pressure, Physical Therapy, 1988, 68, p. 20-25.
(56) ZYLBERGOLD, R.S. and PIPER, M.C., A comparison of three types of tractions, Spine, 1985, 10, p. 867-871.
CONTRIBUTIONS OF COMPILATIONS
(1) SAUNDERS, H.D., Lumbar traction, p. 787-795, In : GRIEVE, G.P., Modern Manuel Therapy of the Vertebral Column, Churchill Livingstone, Edinburgh, 1986.
(2) VALKENBURGH, H.A. and HAANEN, H.C.M., the epidemiology of low back pain, p. 9-22. In : WHITE, A.A. and GORDON, S.L., Symposium on idiopathic low back pain, The C.V. Mosby Company, St. Louis, 1982.
INTERNET
(3) KOKE, A., HEUTS, P., VLAEYEN, J. and WEBER, W., Meetinstrumenten Chronische Pijn. Deel 1 functionele status, Pijn Kennis Centrum Maastricht, Internet (http://www.pijn.com/medici/index5.htm).
LECTURE
(4) DAVID, H., Comparative CT scans in four cases of lumbar discogenic pathology before and after conservative treatment, 5th International Conference IFOMT Proceedings, Vail.
NON-PUBLISHED WORKS
(5) PARIS, S.V., Course notes : Introduction to Spinal Evaluation and Manipulation, St. Augustine FL. : Institute Press, 1989.